
NSCLC 热消融的目标
Patient Selection Criteria
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Patient Characteristics |
ACOSOG – z4033
|
|
High Risk
Limited Recurrence
Cyto-reduction Local Control Refractory Patient Refusal |
Major criteria (1) |
|
FEV1 ≤ 50%
DLCO ≤ 50%
|
|
|
Minor criteria (2)
|
|
|
FEV1 51-60%
DLCO 51-60%
Age ≥ 75 years
Pulmonary hypertension
Left ventricular function (EF ≤ 40%)
Resting or exercise arterial pO2 < 55 mmHg
pCO2 > 45 mmHg
|
|
基本概念 Key concept
理由之一:年龄大的患者治愈性手术切除不获益
Similar Long-term Survival of Elderly Patients w/ NSCLC Treated with Lobectomy or Wedge Resection within the SEER Database
- SEER database; 14,555 stage I /II NSCLC
- No curative (lobar or sublobar) resection
| Age-groups | No resection rate |
| All | 15.7% |
| < 65 years | 7.7% |
| 65-74 years | 14.1% |
| > 75 years | 30.4% |
理由之二:早期或不可切除肺癌,仅仅观察处理预后差
| 治疗方式(例数) | 中位生存期(M) |
| Surgery (43) | 46.2 |
| Radiation (36) | 19.2 |
| No treatment (49) | 14.2 |
No treatment group:14 refused treatment
Cause of death =
cancer in 53% patients (compared to 43% after radiation)
cancer in 53% patients (compared to 43% after radiation)
McGarry et al.Observation-Only Management of Early Stage, Medically Inoperable Lung Cancer Poor Outcome Chest 2002; 121:1155-1158
临床上在选择热消融患者的时候有三种场景:定义治疗;补充治疗和姑息治疗三种理由之三:不可切除早期NSCLC病人的结果和特征
97 patients stage I/II NSCLC(早期)
Cancer-specific therapy (rad/chemo) used in only 27
Median survival 22 months for treated group
Median survival 11 months for untreated group(97-27=70)
根据以上三个理由:选择热消融
1. >70岁,可治愈性外科切除的,(可切除的I/II期)-
2. 不可切除的早期(I/II期)肿瘤,(包括年轻患者,需要和放疗对比吗?)
3. 不可切除肿瘤(应该有大小之分,大的不可切除的肺癌,需要射频局部控制吗?)
根据以上三个理由:选择热消融
1. >70岁,可治愈性外科切除的,(可切除的I/II期)-
2. 不可切除的早期(I/II期)肿瘤,(包括年轻患者,需要和放疗对比吗?)
3. 不可切除肿瘤(应该有大小之分,大的不可切除的肺癌,需要射频局部控制吗?)
1. 定义治疗包括
- Stages I or II with clinical comorbidities
- Stages I or II when the patient refuses Surgery
- Limited number of metastases
Vogl TJ, Eur J Radiol 2011;77(2):346-57.
Abbas G, et al. Surg Oncol 2009;100(8):645-50.
Matsuoka T, et al.Int J Clin Oncol 2007;12(2):71-8.
Casal RF, et al. Clin Chest Med 2010;31:151-163.
De Baère T, et al. Cardiovasc Intervent Radiol 2010;34(2):241-51.
Definitive Therapy:NSCLC
 |
 |
 |
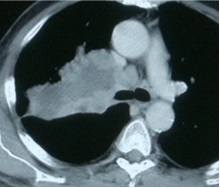
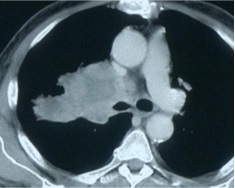
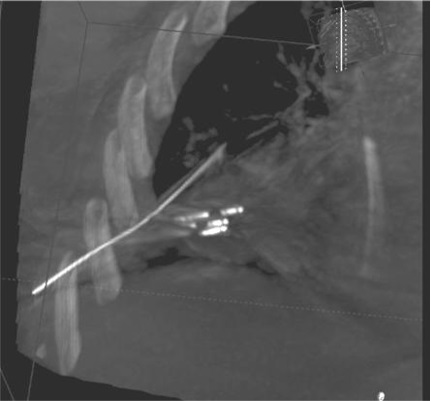
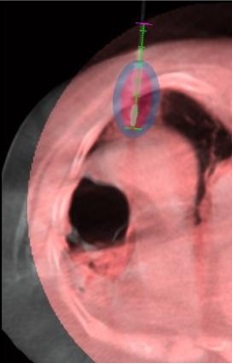
2. Complementary to Other Therapies
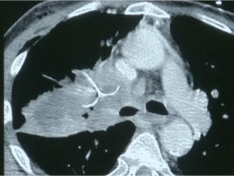
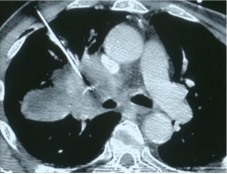
Persistent, solitary, peripheral focus after definitive radiation, surgery and chemotherapy
化疗后残余癌,射频消融(Olympus)
化疗后残余癌,射频消融(Olympus)
 |
 |
 |
 |
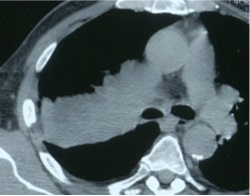
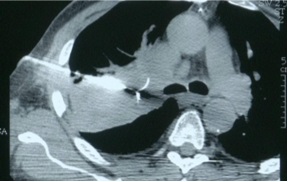
3. 姑息治疗
- Chest wall pain
- Plexus Involvement
- Hemoptysis
- Dyspnea
Lee JM, et al. Radiology 2004;230(1):125-34.
Belfiore G, et al. AJR Am J Roentgenol 2004;183(4):1003-1.
Simon CJ, et al. Radiology 2007;243(1):268-75.
Belfiore G, et al. AJR Am J Roentgenol 2004;183(4):1003-1.
Simon CJ, et al. Radiology 2007;243(1):268-75.
VanSonnenberg E, et al. AJR Am L Roentgenol 2005;184(2):381-90.
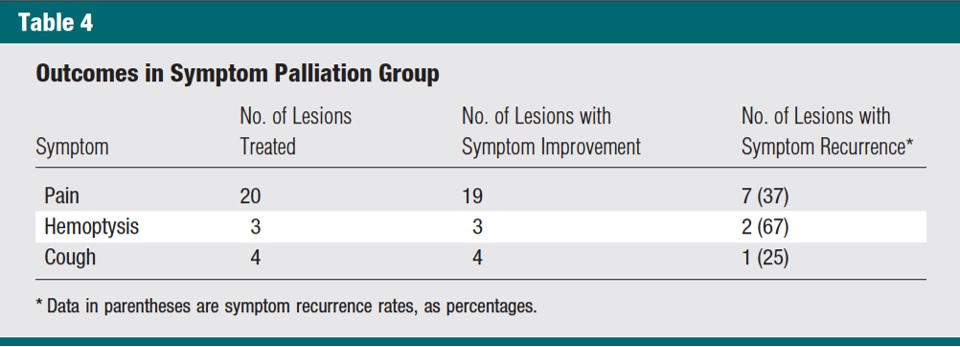
Symptom palliation
 |
 |
 |
|
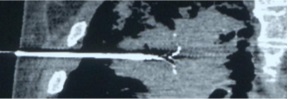
| Palliation for Hemoptysis | RFA 1 |
 |
 |
 |
|
| NSCLC | RFA2 |
 |
 |
| 一个月后 | 咯血停止 |
 |
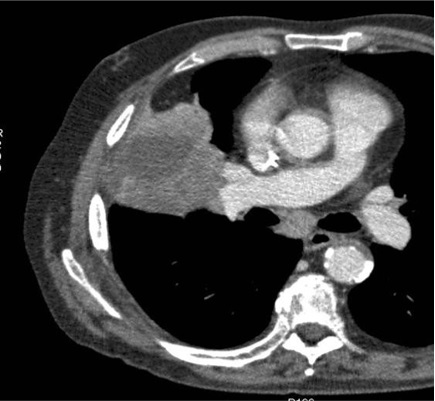 |
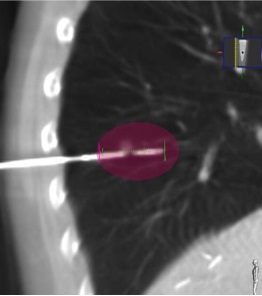
| Palliation for Pain Reduction | NSCLC |
姑息治疗:Treating Pulmonary Metastases:三种场景,低外科手术风险;高外科手术风险;复发性肺转移
Metastases are resectable when:
Primary cancer is controllable/controlled.
Extrapulmonary disease is controllable/controlled.
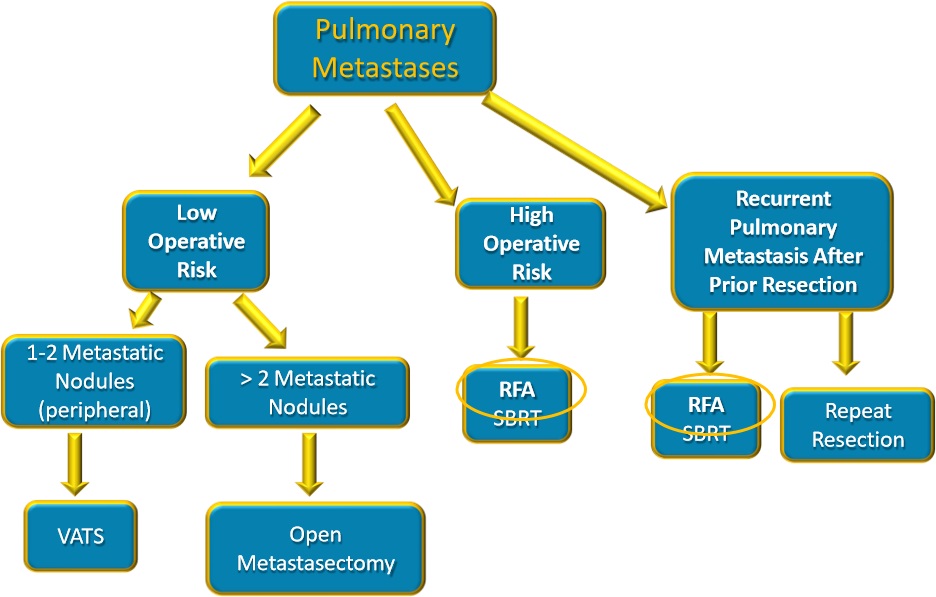
Zheng Y, et al. Surgical and Nonresectional Therapies for Pulmonary Metastasis Surg Clin N Am 2010;90:1041-51.
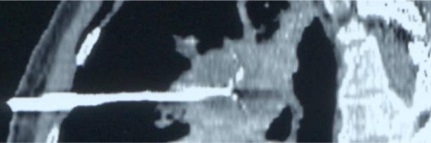
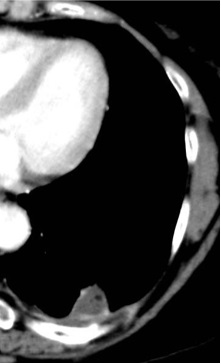
姑息性治疗 : Recurrence after resection
Metastasis Recurrence from Cholangiocarcinoma
 |
 |
 |
除了 1. Definitive Therapy;2. Complementary to Other Therapies;3. Palliation
经皮消融还需要影像学的标准
PERCUTANEOUS ABLATIONS
Imaging Criteria:影像学的标准与 Feasibility 和 Predictivity 相关
Fernando HC, et al. Ann Thorac Surg 2008;85(2):S780-4.
Carrafiello G, et al. Int J Surg 2008;6:65-9.
Vogl TJ, et al. Eur J Radiol 2011;77(2):346-57.
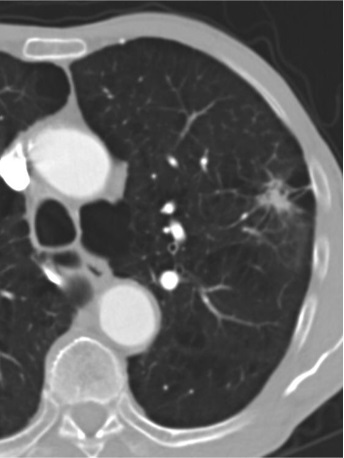
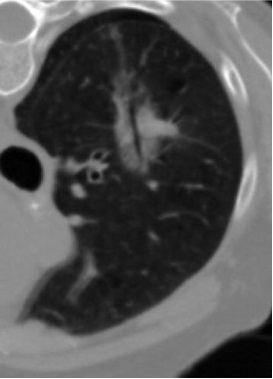
1. Lesion Size
2. Lesion Localization
3. Maximum number of lesions/lung
1)Size
Lesion maximum diameter
- < 3cm – ideal diameter
- it’s accepted that is not possible to achieve complete ablation for lesions > 3,5 cm with RFA, even with mutiple ablations
尽管多针射频,公认不可能实现完全消融的>3.5cm的病变
尽管多针射频,公认不可能实现完全消融的>3.5cm的病变
- MWA – to prefer for lesions > 3 cm (multiple antennas)
Fernando HC, et al. Ann Thorac Surg 2008;85(2):S780-4.
Carrafiello G, et al. Int J Surg 2008;6:65-9.
Vogl TJ, et al. Eur J Radiol 2011;77(2):346-57.
De Baère T, et al. Cardiovasc Intervent Radiol 2010;34(2):241-51.
Herrera LJ, et al. J Thorac Cardiovasc Surg 2003;125(4):929-37.
Roy AM. Curr Probl Diagn Radiol 2009;38(1):44-52
Herrera LJ, et al. J Thorac Cardiovasc Surg 2003;125(4):929-37.
Roy AM. Curr Probl Diagn Radiol 2009;38(1):44-52
Gillams AR. BMJ 2007;334(7602):1056-7.
Gillams AR. Cancer Imaging 2008;8 Spec No A:S1-5.
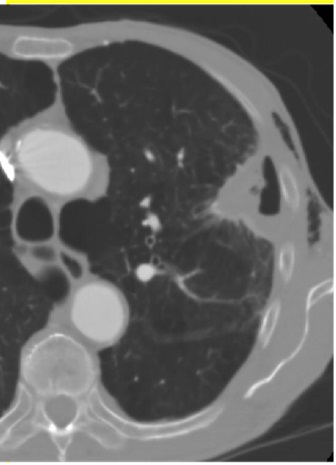
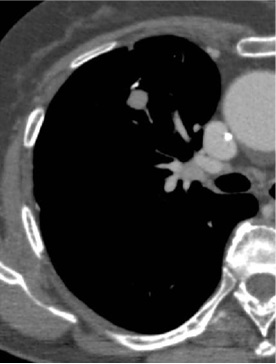
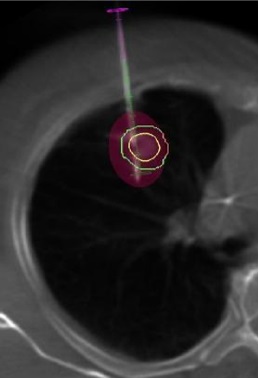
2)Localization
Should not be treated lesions close to large vessels, heart or trachea
- To avoid lesions < 1cm from hilum
- Iguchi et al. – 42 cases at < 10 mm from heart or
- aorta without any complications
- MWA could be better in those cases
LeVeen RF. Semin Inter Radiol 1997; 14:313-324.
Wolf F et al Radiology 2008;247:871-879.
Wolf F et al Radiology 2008;247:871-879.
Gómez FM, et al. Clin Transl Oncol 2009;11(1):28-34.
Lee JM, et al. Eur Radiol 2003;13: 2540-7.
Lee JM, et al. Eur Radiol 2003;13: 2540-7.
Gillams AR, et al. Cardiovasc Intervent Radiol 2005;28:476-80
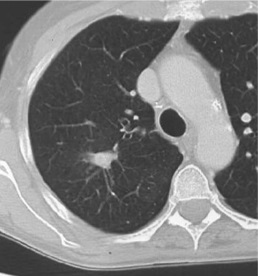
3) Maximum number of lesions/ lung
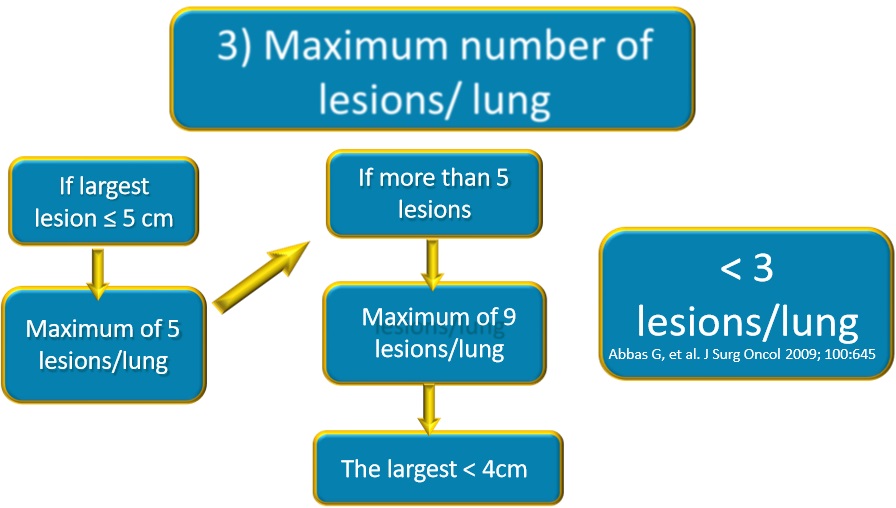
Gillams AR. Cancer Imaging 2008;8 Spec No A:S1-5.
Multiple Lesions
Primary Cancer controlled. No extrapulmonary disease.
Multiple Lesions
Primary Cancer controlled. No extrapulmonary disease.
Metastasis
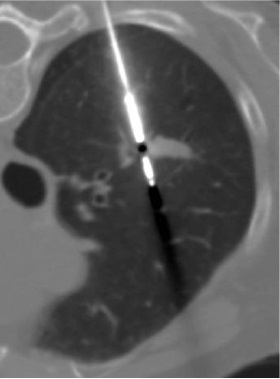
 |
 |
| 俯卧位,后位进针 | 复查(仰卧位) |
 |
 |
Literature Review
- 24 thermoablation studies (23 RFA and 1 MWA) with exposure of selection criteria
- 2003 to 2010
- 1.013 Patients, 605 Primitives, 408 Metastases
|
Literature Criteria |
N of studies (n=24) |
Literature Criteria |
N of studies (n=24) |
|
Pretreatment reccomendation |
|
Imaging criteria |
|
|
- Biopsy |
12 |
Limit value for lesion’s diameter |
11 |
|
- Coagulation disorders |
9 |
Extension of local disease |
19 |
|
- Specialist responsable of the choice |
12 |
Maximum Diameter |
11 |
|
Clinical criteria |
|
Localization (close to major vessels, heart, trachea, hilum) |
19 |
|
- Poor lung function |
19 |
Failure of conventional therapy |
17 |
|
- Comorbidity |
17 |
Surgery Refusal |
18 |
|
- Advanced age |
4 |
|
|
Patient selection conclusion
Curation - complete tumor destruction (R0-like)
Inoperability
Visibility of the tumor target
Abscence of remote metastases (staging!)
Palliation - macroscopic cytoreduction
Pain relief
Decompression